ROI – A Smart Investment
Not so many years ago, locum tenens physicians were a rare breed and demand for their services on behalf of hospitals and clinics was minimal. Times have changed.
ROI Article – Locum Tenens: A Smart Investment
Not so many years ago, locum tenens physicians were a rare breed and demand for their services on behalf of hospitals and clinics was minimal. Times have changed. All around the country, in rural and metropolitan areas alike, physicians shortages and long recruitment cycles have become the norm. Do any of the following scenarios sound familiar to you?
- For the third time in less than a month, you’ve had to close one of your hospital’s operating suites due to lack of anesthesiology coverage. The group that covers your facility has been trying to recruit new associates for some time now, but the shortage in the specialty is making it tough. They don’t want to settle for anyone less than top-notch, and you don’t want them to. But hearing about your “loyal” surgeons taking cases to the hospital across town and seeing the weariness in the eyes of the anesthesiologists you do have on staff is making you nervous. How much longer can this go on without seriously impacting revenue, not to mention your institution’s reputation as a full-service facility?
- Recession or no recession, your practice has never been busier. The four doctors and two nurse practitioners on staff are working at capacity and, although they’re not complaining (yet), as the practice administrator you are wondering if it’s time to recruit a fifth physician. At the same time, you question whether or not patient volume is growing rapidly enough to support another full-time doctor’s salary, not to mention expenses and benefits. You don’t want to bring in a new associate only to have him or her sit around for months waiting for the schedule to fill. If only you could test the waters to find out if the adage “if you build it they will come” would hold true in your situation.
- Your ER group has always had a stellar reputation for providing quality care and received high marks for patient satisfaction. But looking over the statistics for last quarter has you shaking your head. Patient wait times are up, incident reports have climbed in number (and you suspect seriousness), one of your key doctors is going part-time as of next month when her baby arrives, and another gave notice citing acute exhaustion from working too many shifts. You need help and you need it now. But qualified ER doctors aren’t exactly standing on street corners looking for work. Indeed, recruiting has become one of the most challenging aspects of your job.
- As a solo practitioner in a rural community, you find it difficult to get away from your practice for more than a few days at a time. Overhead continues even if you’re not there to generate revenue and patients have to go without care or travel long distances to see another doctor if you are not available. But you need a “real” vacation – and soon. You’re dreaming of backpacking around Europe and your husband has been researching what it would be like to work with a volunteer organization in Africa for a month – or longer. You keep telling yourself that you only live once and that you should take advantage of all that life has to offer, but your more practical side wonders how you can get away for an extended period and still have a practice to come back to.
- Your only full-time radiologist has had emergency surgery and will be out of commission for 3-4 weeks. A colleague at another hospital had mentioned their use of “tele-radiology” so you give her a call to get the details. She says it’s a viable option... if you can afford to pay $60 per study read. In your case, the cost would be more than $5,000 per day. Back to the drawing board.
- As managing partner of your practice, you’ve been searching for the perfect OB/GYN to join your group for one full year. During this time you’ve turned away dozens of obstetrical patients, watched with regret as primary care physicians referred patients to the next town over for surgical consultations, and listened to even your most loyal patients complain about having to wait months to schedule a routine annual exam. During this one year, your practice has left close to $600,000 in collections on the table while your primary hospital has missed out on well over $1.5 million in gross billing.
Paging “Doc Hollywood”
Page all day long, but don’t stand on one foot waiting for a response. Baby boomers were among the first group of physicians who did not customarily take a position or open a practice right out of training and stay there until retirement. Gen-X doctors, having watched their own parents change jobs and make geographic moves throughout their working lives, are even less likely than their mid-career colleagues to remain in a single location for the duration. Add to this the fact that the physician shortage is in full swing in many specialties and likely in the making for many others. The number of residents currently in training in several key specialties – anesthesiology, cardiology, emergency medicine, family practice, general surgery, internal medicine, OB/GYN, orthopedics, and radiology – are lagging far behind when compared with physicians in those same specialties who are over the age of 55. Is this a “perfect storm” for the future of physician recruitment and retention? Quite possibly.
Locum Tenens to the Rescue?
Locum tenens coverage can solve all of the problems referenced in the scenarios above. And yet, there is still hesitancy on the part of hospital and medical practice executives about making use of this valuable resource. By far, the most common objection to engaging locum tenens physicians is the cost. Paying more than a thousand dollars per day for physician coverage is a hard pill to swallow for those who keep a close eye on the bottom line. What many healthcare executives don’t realize, however, is that in most instances locum tenens physicians more than pay for themselves in terms of professional service revenue (physician billing) and inpatient and outpatient revenue generated for their affiliate hospital.
For every hospital administrator or clinic manager who thinks that locum tenens physicians are too expensive, there are many others who have discovered the bottom line benefit of using temporary doctors. Consider the numbers for ten specialties.
Note that the table does not take into account the significant inpatient and outpatient revenue that a physician in any of the ten specialties generates each day by ordering diagnostic tests, therapeutic services, performing surgery, delivering babies and tending to hospitalized patients.
In addition to the locum tenens physician’s daily rate, you will pay for travel and housing and extra for overtime and on-call duty. But, when you consider that you’re not paying the employer’s portion of FICA, benefits, malpractice premiums, and CME expenses and suddenly using temporary physicians starts to look rather attractive. Factor in the non-monetary benefits of having proper physician coverage, and locum tenens quickly moves into the “smart investment” category.
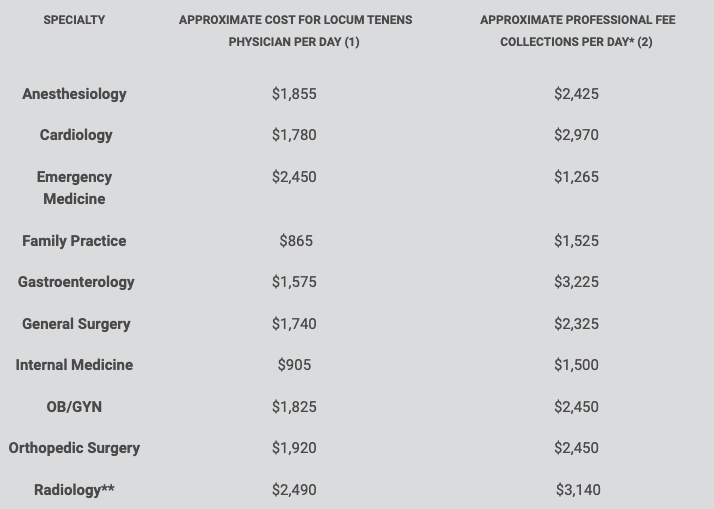
(1) Source: Average of several locum tenens agency rates. (2) Source: MGMA Physician Compensation and Production Survey: 2008 Report Based on 2007 Data ** MGMA provided collections per week; article assumes 5-day work week. **Average for invasive and non-invasive.
More to the Equation than Money
Aside from the bottom line, there are several issues that make utilizing locum tenens physician a sensible investment. Patient and referring physician satisfaction and physician retention are among the most important.
Patient satisfaction. Patients are more educated, savvy, and – yes – more demanding than ever before. They have high expectations when it comes to their medical care. If a patient can’t get in to see a doctor in a timely manner, has to wait for hours in the local hospital ER, or is told that their elective surgery has to be rescheduled because there is no anesthesiologist available they quickly become dissatisfied. Patients in these situations are likely to vote with their feet and seek care elsewhere or, at minimum, share their tales of woe with friends and family members. Healthcare administrators interested in maintaining high patient satisfaction ratings as well as their fair share of the market should consider making locum tenens coverage part of an overall medical staff strategic plan.
Referring physician satisfaction. Like patients, referring physicians expect full-service, high-quality care for their patients. They want their radiology reports delivered in a timely manner and they want the comfort of knowing that if they need a cardiology consult at 3:00 a.m. on a Sunday morning that they can get it. Locum tenens coverage can solve access problems before they get out of hand.
Physician retention. With serious shortages in so many specialties, physicians are in the position to “just say no” if the demands of practice outweigh the rewards. Younger physicians in particular insist on reasonable schedules and enough time off to keep themselves from becoming exhausted and slipping into professional burnout. They want life balance which means not being on call every other night or every weekend. Providing your permanent physicians with locum tenens coverage on a regular basis so that they have time for rest and renewal is one tactic to retain the physicians you’ve worked so hard to recruit.
Astute hospital and clinic administrators now realize that retaining the physicians they have should be the highest priority if they don’t want to spend half their time looking for new doctors year after year. Making sure that your busiest doctors get several weeks off each year by using locum tenens physicians may be the best investment you can make in terms of retention. Exhausted, overwhelmed, burned out physicians tend to be unhappy, make those who work around them equally unhappy, and may not have the level of resilience required to provide the highest quality care.
Other “non-money” benefits of maintaining full physician coverage include the ability to stay in compliance with managed care and other third-party agreements, fewer scheduling upsets, and less stress on front-line office staff (yes, constantly saying ‘no’ to patients in need is stressful).
Recruitment Costs
It is estimated that the cost to recruit a physician can reach three to four times that physician’s annual salary. This includes actual recruitment costs plus lost revenue during the period of time it takes to find, relocate, and orient a new physician.
Maximizing ROI
Once you’ve made the decision that utilizing a locum tenens physician makes sense for you, there are steps you can take that will ensure the greatest benefit – monetarily and otherwise. Here are four steps to consider.
(1) Plan ahead. Organizations that utilize locum tenens physicians on even a semi-regular basis have learned the advantage of planning strategically and well in advance for their physician needs. Savvy administrators look ahead and ask: Who is taking an extended vacation? Who will be out on maternity leave? When does “peak season” begin and end in our area? Locum tenens agencies are more likely to find your “perfect match” when they have sufficient time to work on the placement. Of course, emergencies arise that make is necessary to bring in a locum tenens physician on short notice and recruiters routinely fill positions on that basis as well. You may end up paying a premium to secure a suitable candidate on short notice, however, so, let your locum tenens agencies know about your needs as soon as possible so that they can make the best physician match for you.
(2) Provide orientation. When you are paying $900, $1,500, or even $2,000+ per day for a physician’s service, the natural tendency is to want to put him or her to work the moment they arrive. That’s possible in some settings, but in most cases a few hours or even a full day or orientation will ultimately increase a physician’s productivity. Locum tenens practitioners should know “who’s who,” where to find the supplies and equipment they need, how to use the electronic medical records system and other technology, where to go with questions, and even basics such as the location of the physician’s lounge, cafeteria, and medical library. Investing in orientation pays off in the long run.
(3) Schedule appropriately. Once a locum tenens physician is properly oriented, schedule them for maximum return on investment. This does not mean double booking them from morning until night, however. Communicate honestly with your locum tenens agency at the outset about patient volume. Some internists are comfortable seeing 20 patients each day while others have a practice style that makes taking care of only 12-14 per day feasible. This often depends on the acuity level of the patients in the practice, so factor that in when you request a locum tenens physician. Once it’s known what the ideal patient load is for a particular physician, make sure he or she is booked to see that number of patients each and every day. Allow for the fact that to a locum tenens physician each patient is “new” and that they will need a little time to become familiar with the nuances of charting, coding, and other paperwork in your location. Always take care not to overbook a locum tenens physician to the point that it might compromise patient care or satisfaction.
(4) Know how to bill for locum tenens physicians. “Locum tenens” is Latin and means “holding one’s place.” When a locum tenens physician is legitimately in that position (i.e., filling in while another doctor is on vacation, sabbatical, or medical leave) in most instances a hospital or clinic can bill for the locum tenens physician’s (but not a CRNA’s) services using the permanent doctor’s provider numbers. If a locum tenens physician is covering while a group is in recruiting mode or to help out during seasonal spikes in patient volume, then the locum tenens doctor is not “holding one’s place” and therefore needs his or her own provider numbers for billing purposes. When a locum tenens (or any physician) begins seeing patients before their Medicare/Medicaid provider number applications have been processed, there are special modifier codes that can be used for billing. Work closely with your billing supervisor or outside billing agency to determine how to use special codes, bill retroactively, and otherwise make sure that locum tenens physician services are reimbursed by third party payers. Try not to get frustrated and simply give up on billing for locum tenens physician services, even if it means extra paperwork. Proper billing can make the difference between a temporary physician being a cost center and a revenue center.
Billing Resources
www.caqh.org – Universal Credentialing Datasource ®
www.medicare.gov – Search for provider application forms 855- R and 855-I
You Are Not Alone
If you are using – or considering using – locum tenens practitioners in your facility you are far from alone. NALTO® estimates that three-quarters of all hospitals now use locum tenens physicians to augment their permanent medical staff. Temporary physicians provide patient care for a total of more than 600,000 days per year. The locum tenens business has grown into a $1.9 billion industry. Twenty years ago misconceptions swirled about locum tenens doctors – that the quality of care they provided was not “up to par,” that they were largely semi-retired and “hanging on” for a few extra years of income, or that physicians did locum tenens because they were unqualified for a “real job.” Those myths have long since been dispelled and hospital administrators and clinic managers who routinely use locum tenens physicians know that they are among the best trained, most personable, and well rounded individuals in their field. Locum tenens doctors tend to be flexible, engaged, and happy with their careers. All of this adds up to good patient care and good working relationships with other doctors and support staff.
Astute healthcare executives now realize that utilizing locum tenens physicians has many benefits. Consider adding locum tenens to your long-term physician relations strategy. It may just turn out to be a very smart investment.
Physicians & Facilities
Upcoming Events